
Dudley Do-Right
On June 30, 1969, I officially finished my four-year residency in Pathology at The Mount Sinai Hospital, New York. The last week was vacation time, enabling me, on July 1, 1969, to begin my two years as “Chief, Laboratory Service” at the Naval Hospital in Beaufort, South Carolina.
This was fifteen months after the Tet Offensive, a massive series of surprise attacks by the North Vietnamese Army and the Viet Cong. Launched during the Vietnamese Lunar New Year (Tet) holiday, it had surprised the American and South Vietnamese forces.
The Tet Offensive was directed against allied cities, towns and military installations in various parts of South Vietnam. The Tet Offensive ultimately was a crushing defeat for the North with many casualties on both sides. But it proved to be powerful strategic psychological victory by demonstrating the capabilities of the North, leading to an erosion of public and political support for the war in the United States. Despite heinous acts by the Nixon administration, including the murders of innocent students at Kent State University by National Guard troops sent there to “keep the peace,” there would be resultant shifts in United States policy and eventual withdrawal from South Vietnam.
“Dudley” is a male given name, derived from the Old English place name meaning “dry field.” It is also a borough in central England, near Birmingham. Robert Dudley was a favorite of Elizabeth I and is thought to have been her lover. Thomas Dudley was an English governor of the Massachusetts Bay Colony in the early 17th century. Dudley Dursley is a Muggle and the bullying cousin to Harry Potter of the enormously popular J.K. Rowling series of books. I’ve known a few highly successful people with the name Dudley.
“Dudley” is also the pejorative term often applied to someone who is dim-witted and hopelessly inept, but well-meaning and conscientious, as exemplified by the Bullwinkle character, Dudley Do-Right of the Mounties.
What are the ties linking the Tet Offensive, the Naval Hospital in Beaufort, South Carolina and someone called Dudley?
The first may be obvious. My two years in the military were not entirely voluntary. I had signed up to the “Berry Plan” in 1963, while a second-year medical student. The Berry Plan was a program that allowed young physicians to complete their education after medical school, as residents and fellows, simultaneously allowing the Department of Defense to know that they could count on the necessary number of specialist physicians for the coming years. It also gave medical students the opportunity to select the service they wanted—I selected the United States Navy—and be eligible for summer clerkships in military hospitals and other health care facilities. You could also sign up for the Public Health Service and have similar, but fewer, choices. If you were willing to commit to more than two years in the military you could be paid a salary while still in medical school.
Although I definitely could have used extra money in those years, managing to finish medical school only because of a scholarship I received in my third year as well as the financial support of my parents and Kate’s father, I was unwilling to commit to the more than two years required if you received monies before being called to active duty. I had attended a few anti-war rallies and was torn between being a pacifist and being what was then thought of as patriotic.
Kate and I discussed moving to Canada if I was to be assigned to duty in Vietnam. I was called up in March 1969 and ordered to report in July to the Naval Hospital, Beaufort, South Carolina, beginning July 1.
Beaufort, South Carolina, is a charming town along the Beaufort River, separated from the Atlantic Ocean by a series of small islands. Beaufort is approximately halfway between Charleston, South Carolina, and Savannah, Georgia. South Carolina and Georgia were the only states of the original 13 to have open policies towards Jews and there was a small but thriving Jewish community in Beaufort. Although we are not observant and do not share key religious beliefs of Judaism, we do love the history and traditions and cherish the concepts that life is all important and that it is our responsibility to make the world a better place. I would not have grieved had I been in a place without a Jewish tradition but it was comforting to be in a place where Jews were a part of the fabric of the community.
I briefly wrote about Beaufort in previous blog posts (https://stephenageller.com/2023/10/28/thoughts-on-seeing-a-rabbis-recent-sermon-about-the-recent-brutal-savagery-in-israel/; https://stephenageller.com/2020/12/16/beethovens-250th-a-half-century-of-celebrations/ ; https://stephenageller.com/2020/10/12/on-listening-to-chopins-g-minor-ballade/ ; https://stephenageller.com/2023/02/18/the-greatest-jazz-pianist/).

Naval Hospital Beaufort, South Carolina
The Naval Hospital had been built in the shape of an anchor and the Chief of the Internal Medicine department at the Naval Hospital was someone we all called “Dudley”. I was the only pathologist at the hospital. Indeed, I was the only pathologist in Beaufort County, often called on to provide assistance to the physicians at the local hospital, Beaufort Memorial.
Dudley was one of three Internists. No one called him that name to his face but it was the only way we referred to him when he wasn’t around. I don’t remember his real name. The other two specialists in internal medicine were reservists.
Paul J. (“Jugger”) and Noel W. were serving two-year terms, as I was, and, beginning a few weeks before, on July 1, had completed one year and were now considered “short timers.” We all knew we were fortunate to be in Beaufort and not Vietnam. Jugger and Noel had been residents together, at Washington University in St. Louis. Noel had, as far as I knew, been assigned to Beaufort by chance but Jugger had requested it to be close to his family home in Savannah. When I think of the best doctors I have known in my seven decades in medicine, Jugger and Noel W. are high on the list.
Years later, when thinking about those days, I concluded without any evidence, that those two exceptionally skilled physicians had been assigned to our somewhat remote facility, rather than some high-powered Naval Medical Center such as those in Bethesda, Maryland or San Diego, California (both of which I had requested), in order to protect the military community of Beaufort from Dudley.
Dudley was regular Navy. He had the relatively high military title of Commander because he had already put in more than 20 years in the Navy. Navy ranks ranged from Ensign (think of Jack Lemmon as ensign Pulver in the wonderful film “Mr. Roberts,”), to Lieutenant junior grade, Lieutenant (Henry Fonda as Mr. Roberts), Lieutenant Commander (the rank I and other reservists had), Commander, Captain and then two levels of Rear Admiral, Vice-Admiral and Admiral. Dudley had no plans to retire and, before we left Beaufort at the end of June 1971, he would be promoted to Captain.
My first interaction with Dudley was in mid-July, during my first weeks at the hospital. I was in my office catching up on some administrative work, rendering diagnoses on biopsies and resection specimens and reviewing the weeks PAP smear slides. PAP smears are glass slides prepared from swabs of the uterine cervix and vagina. They are an exceptionally useful way of detecting early cancers of the female reproductive tract, based on research from the 1920’s by Georgios Papanikolaou (1883-1962), a Greek immigrant to the United States who was a physician, zoologist, and microscopist working at Cornell Medical College in New York City. In most settings, PAP smears are microscopically studied (“screened”) by a skilled cytology (cyto = cell) technician, who identifies all suspicious cells for review by a cytopathologist who then provides the ultimate diagnosis. There was no position of cytology screener at Naval Hospital, Beaufort, and it was my responsibility to both screen the slides and make diagnoses. A PAP smear typically includes hundreds of cells, each of which must be individually studied.
Each week there were many PAPs to review. Although Beaufort’s native population was only 9,000+ people, the community had more than 50,000 occupants during the Vietnam years, including military people, spouses (in those years, almost all wives) and children as well as civilian employees of the various military posts. There were a small number of family members for the physicians, technicians and varied hospital employees but the two nearby Marine facilities, Parris Island recruit training base and the Marine Air Station, accounted for many of the dependents. There were also many retired military people.
Reviewing PAP smears is, for me, very tedious work. Fortunately, most of the women in the community were young and
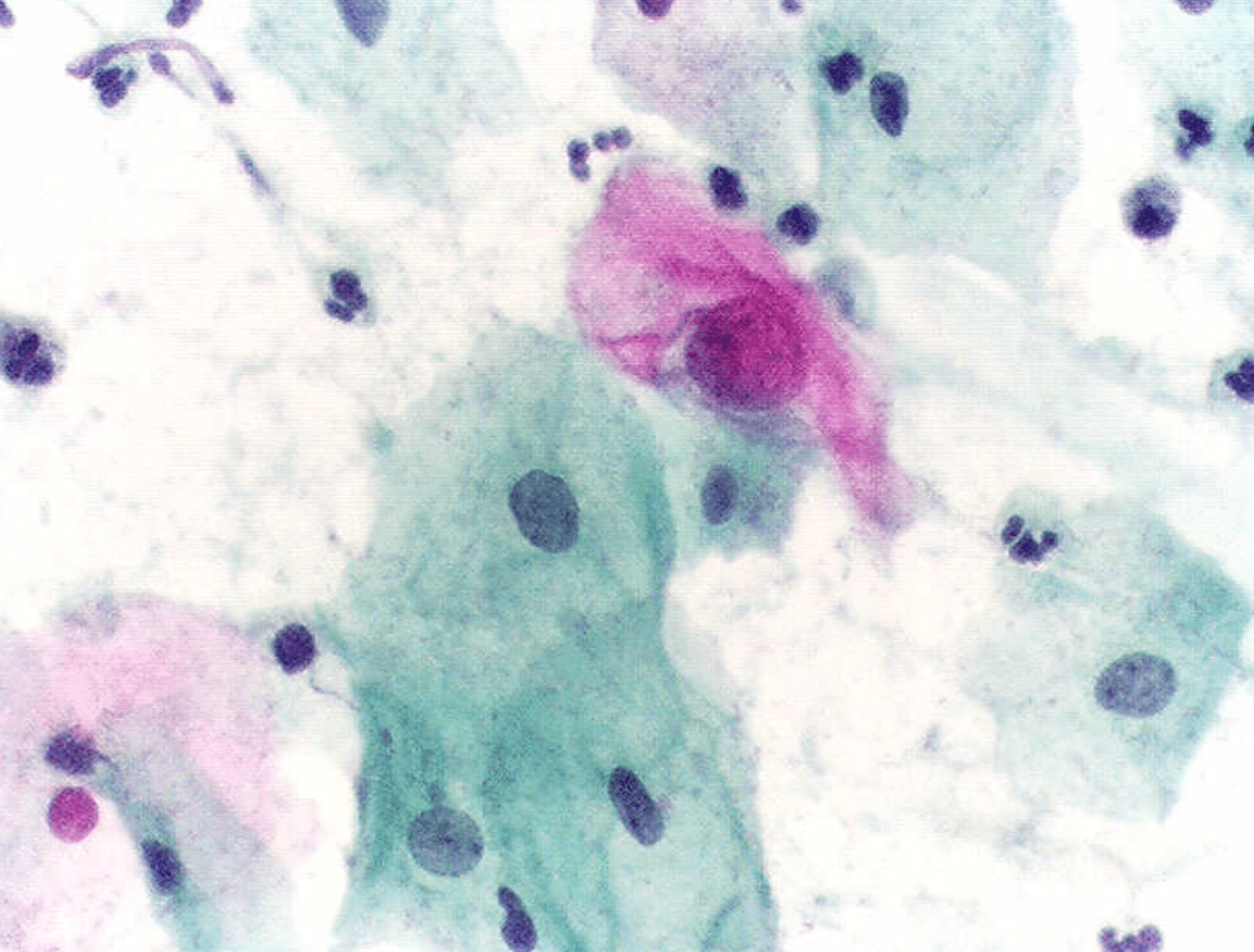
high magnification microscopic image of PAP smear
their PAP smears were usually unremarkable. Unfortunately, looking at unremarkable PAP smears is exceedingly boring and it became my practice to review smears from any woman older than 25 twice to make sure I didn’t miss something important. I did find an abnormal PAP ever now and then, usually in an older woman, which reassured me that I was doing okay, but I always wished there was someone else also checking those slides. After almost a year of campaigning, including many letters to BuNav (the Bureau of the Navy), we were eventually approved for a screener, making my life considerably easier and more tolerable.
On this late July afternoon, I was at my microscope studying slide after slide when one of the laboratory technicians knocked on the door. He had two red-top blood-filled test tubes in his hands, holding them out for me to see.
“Doc, I don’t understand why these tubes won’t clot.”
Most blood tests are performed on tubes with and without anticoagulants. Blood, mixed with an anti-coagulant so it can’t clot, in tubes with purple tops, allows you to study the various blood cells and solid components, such as red and white cells and blood platelets. The clotted blood (red top tubes) is centrifuged to have all the solid elements at the bottom of the test tube and the clear, unclotted portion (“serum”) at the top. The serum is used to study the various chemical components (glucose, calcium, sodium, potassium, etc.).
I remember that I literally jumped from my chair, took the red top tubes from him, shaking them myself to confirm that they were, indeed, unclotted, and said, “Let’s go look at the patient. Show me where she (the label on the tube gave her name, age, sex and hospital number) is.” I was still relatively unfamiliar with the hospital layout and followed him to the nearest staircase, urging him to go as fast as possible. “She probably has D.I.C..”
“What’s that?”
D.I.C. is disseminated intravascular coagulopathy, also known as disseminated intravascular coagulation, consumption coagulopathy and other names. In D.I.C., something (trauma, infection, toxin, immune response) triggers the formation of a clot somewhere in the body. For various reasons, the clot, which can be quite small, absorbs all the fibrinogen (a substance produced by the liver and released into the blood, necessary for normal, healthy blood clotting, including sealing of tiny blood vessel defects that normally occur). When there is no fibrinogen, uncontrollable bleeding, without mechanical trauma, occurs. This explanation, and the elaboration below, is highly simplified in this essay because it is so complex and complicated it would take many pages to depict.
Mary F. (not her real name), 34 years old, was comatose in the I.C.U. bed closest to the nursing station, bleeding from every orifice: mouth, nose, ears, gums, vagina and intestines. Blood was all over, on the bed clothes, towels, tissues, the floor. I would later learn that she was the wife of a Marine pilot, had three children and had collapsed in her dentist’s chair after receiving a Novocain injection before her intended procedure. Unfortunately, she had an acute, severe allergic reaction, a type of response associated with D.I.C., and the dental office apparently was not approved to have injectable adrenalin, which might have saved her life.
I turned to the nurse. “Who’s the physician on duty?”
She gave Dudley’s name.
“Has he ordered heparin?”
At that time, heparin, a powerful anti-coagulant, was the best treatment. Heparin typically is administered to interrupt clotting but, in D.I.C., it acts on the abnormal focus of clot formation, releasing fibrinogen for its usual function.
Dudley was in his office, down the hall from the patient units.
Me: “Mrs. F. has D.I.C.. She needs treatment right away.”
Dudley: “I ordered a bottle of blood.”
Me: “No. You need to give her heparin. She has D.I.C..”
Dudley (with a somewhat condescending and scornful look): “Uh, no, she’s bleeding. You don’t want to give her heparin.”
Me: “Heparin. She needs heparin. She has D.I.C.”
Dudley (brow now deeply furrowed): “What’s D.I.C.?”
In 1969, D.I.C. was not yet universally known but there had been scientific articles, including review articles, in leading internal medicine journals. A comprehensive textbook devoted to all aspects of D.I.C., including clinical and research, written by Donald McKay, had been published four years before. The major textbooks included D.I.C.. I, and all my fellow residents, read the McKay book soon after it was available. Every internist and every pathologist I knew was familiar with D.I.C..
I started to give Dudley a short summary of the condition but stopped, and just said, “I’ll be right back.”
I ran down the stairs and got on my bike.
Although the official name was the “U.S. Naval Hospital, Beaufort, S.C.” and it is now called “Naval Hospital Beaufort,” it is mostly situated in the neighboring Town of Port Royal, S.C.. The hospital is on 127 acres of land and opened in 1949. During the Civil War the site was the camp for the First South Carolina Volunteers, the initial federally authorized unit of African American soldiers to fight for the Union.
The Naval Hospital Beaufort was one of the few military facilities designated a “compete military compound,” rather than one component of a larger command. Located within the grounds are more than 50 family housing units, on four separate circles, with an abundance of weeping willow and oak trees. There were also two small dormitory-like buildings labeled BEQs (Bachelor Enlisted Quarters, which housed both men and women) and a gas station. Recreational facilities on the property include a swimming pool, lighted tennis and basketball courts, a gym and a children’s playground. There’s also a fishing pier but the tide is typically out leaving the water many feet below the pier. The ruins of Fort Frederick, built with seashells and mortar (“tabby”) in 1732, were directly behind our house, Quarters D, which was on the circle closest to the hospital.
Jugger lived on the same housing circle we did, directly opposite our house.
Fortunately, he was home, playing with his children. Before I finished explaining the situation, he was on his bike and we were racing back to the hospital.
I deliberately waited to the side as Jugger spoke to Dudley and the ICU nurse. The nurse quickly brought the heparin dose to the bedside and Jugger administered it.
The bleeding stopped, literally within a few minutes. Jugger spoke to Dudley again and then came over to me and whispered, “Good job. I’ll be home.”
After the Navy, Jugger went to a fellowship in infectious diseases and then returned home to become the first infectious disease specialist in Savannah, Georgia. In his obituary, 46 years later, he was described as “fearless and a man with unlimited compassion and boundless humor.” His compassion and brilliance served well at the time when AIDS started killing many young men in Savannah.
Before I went home a few hours later I went back to the I.C.U.. All the blood-stained bed clothes had been replaced with bright while sheets and pillowcases. Mary G. was sipping some juice with a straw. She looked fine.
A few hours later, unbeknownst to me, she started bleeding again. This time, Dudley did not administer heparin. I performed the autopsy on Mary G. the following Monday morning.
One of my medical school teachers, the exceptionally gifted surgeon, LaSalle Lefall, would say, “There are only two kinds of mistakes you will ever make; the things you forgot and the things you never learned.” Dudley’s judgement was clearly faulty, in this and other cases, because his knowledge base was significantly deficient.
There are many other examples I could give of how incompetents sometimes succeeded, and even thrived, in the military in those years. Mostly the other doctors I dealt with were, at least, capable and some were outstanding. Peter F. was the Chief of Surgery. It was a privilege to know him and to watch him operate, as I sometimes did. He was a fine surgeon and a wonderful person. Al P. was an excellent Ob-Gyn and became a long-time friend.
Sometimes it was the system that didn’t work, rather than the individual but, as many a novel, play and movie has demonstrated, there is usually some heroic figure around to plug up the hole in the dike.
One small example concerns a camera. On my first day, I realized there were no cameras in the laboratories. I was accustomed to being able to photograph interesting surgical specimens as well as autopsy cases, for both documentation and, more immediately, teaching. One of my teachers in pathology residency was Sadao Otani, who was an extraordinarily gifted pathologist but also a skilled photographer. I also always had a camera for my microscope.
I made an appointment to see George W., the “Exec” (Executive Officer) second to the Commanding Officer in administering the hospital. He was neither sympathetic nor helpful. He informed me that our facility was not authorized for cameras in the Pathology department. Period! I spoke to Pete, the surgeon. When he came across something in the O.R. that he wanted to photograph, he used a camera he kept in his desk. I owned an excellent Konica 35 mm single-lens-reflex (SLR) camera but wasn’t quite ready to donate it to the cause. I went back to my office and, after a few days managed to talk to the Department of the Navy pathologist, in Washington, D.C., who was responsible for the all Navy pathologists. I had met him once and now reintroduced myself. He was sympathetic to my need but, if we weren’t approved for a camera, there was nothing he could do. Period!!
I headed back to my office to tell my secretary (now called “assistant”) I was going out for about an hour. Chief Petty Officer Smith (“Smitty”) was in the office and asked if there was anything he could do to help. A Chief Petty Officer is a senior non-commissioned officer in the Navy. I would soon learn how fortunate I was in having a smart and experienced CPO to work with in the laboratories.
I explained that I was going to the PX (Post Exchange, akin to a small department store for the exclusive use of military people and their families), about 20 minutes’ drive away, on Parris Island, to buy a camera. Smitty asked why I needed a camera.
After I explained, he said, “Come with me.”
We got into his car and drove to the Marine Corps Air Station (MCAS), 20 minutes away, where pilots are taught the art of flying war machines. Think of the “Top Gun” movies for the Navy counterpart. If you want to better appreciate the MCAS, Beaufort, where we went, you should read Pat Conroy’s semi-autobiographical novel, “The Great Santini,” a wonderful book, or see the film of the same name based on the book, starring Robert Duvall and Blythe Danner.
Smitty pulled up to a hangar-like building at one side of the air base. Inside, he introduced me to his counterpart, another “Chief” (the Chiefs all tended to use that title when referring to, or even talking with, one another). Looking around, I could see the building was crowded with a huge collection of “stuff,” including telephones, typewriters, file cabinets, tables and chairs and other furniture, refrigerators, bookcases, lawn mowers, etc etc etc, and cameras. Every imaginable type of camera was there, including aerial cameras, underwater cameras, cameras with telescopes; every known brand (including Hasselblads, Leicas, Nikons, Mamiyas, and many others) was represented and there usually were two or three of each kind. I had been brought up by a father who always had cameras and the sight was, to say the least, impressive.
“These Hasselblads are terrific,” my new Chief friend said.
“Thank you, but I don’t need anything so sophisticated,” I said. (Or, only a few weeks out of New York, I thought, so stealable. I would ultimately appreciate that stealing was a rare event on the Beaufort military bases.) I opted for a reasonably good quality Kodak 35 mm SLR that served me well for the next two years.
“Do I need to fill out a requisition form?”
“Nah. Let me know if you decide you want a different camera.”
I learned that the military is, in many ways, a microcosm of society. You could succeed, as Dudley did, by lasting a long time and staying out of trouble (“keep your nose clean.”). You could also succeed by knowing the right people.
And you could succeed by demonstrating excellence.
The Navy people and the Marines sometimes thought of themselves as rivals. Some of the Navy used to say that the reason the Marines had such high casualties in war is that they weren’t smart enough to duck. I sometimes saw evidence of that in our peaceful setting. Some of the young men coming to the Marine Corps Recruiting Depot (MCRD) at Parris Island had been given the choice of going to jail or joining the Marines. Some of them were not very bright. But some of the recruits had been in reserve units and were in law school or engineering school or some other academic pursuit when their units were called up. Others, including non-commissioned officers and commissioned officers, were as smart as anyone, anywhere. The military often manages to recognize the most capable people and responsible people.
I don’t know what happened to Dudley after Beaufort. Perhaps I shouldn’t make the harsh judgements I have made about him because of that one interaction but he had earned the pseudonym before I knew him and no one thought it a misnomer. I didn’t deal with him very often. Most of the very sick patients seemed to be under the care of Jugger or Noel W., who I interacted with regularly because of patient needs. One or the other would come to my office to discuss laboratory results or review a biopsy.
I have only the faintest recollection of the two internists who replaced Jugger and Noel W. when they left the Navy in June 1970. By then, there was a screener and much of my concentration was devoted to preparing for the examination by the American Board of Pathology that I would be taking for Board certification. I was also looking for a job for the following July, 1971, when I would no longer be a naval officer. As it turned out, I would go back to Mount Sinai, not exactly what I was planning but, as it turned out, one of the best things that ever happened to me. That’s another story for another day.
I also was involved in helping my young associate, Lieutenant John Maples, a non-physician MSC (rather than being in the Medical Corps as I was, he was in the Medical Service Corps) who, along with Smitty, managed the labs.

Blood typing instrument printout – the red marks represent interaction of blood types and specific reagents
A brilliant technologist, John elected to make the Navy his career and went on to earn a Ph.D. in Immunology, Maples was the person responsible for the various testing instruments in the laboratory. On my first day he brought me down to a basement storeroom and showed me abut a dozen large, unopened shipping boxes labeled “Technicon.” He informed me that we were tasked with putting together one of the first automated blood typing instruments in the country, to meet a Department of the Navy directive. Each week, beginning in a few weeks from that day, Marine recruits would “volunteer” to donate a unit of blood and determine the blood type and other characteristics. The next day, the blood would be shipped to San Francisco where it would be tested again to check on our work (we never made an error!). A few days after that, the blood would be shipped to Vietnam.
It was the only time in their entire ten-week training period when those recruits would get a Coke or other soft drink.
At first, we drew the blood in an empty barracks on Parris Island. But, in addition to requiring us to ship all our equipment there, there was no air conditioning and the facilities for drawing blood were exceedingly poor. Eventually, I was able to convince both the Navy and the Marines that we couldn’t guarantee that the blood units weren’t going to be contaminated by the sweat of those young men when it inevitably ran down their arms and onto the needles in their veins. It was agreed to transport the recruits to an unused ward at our hospital for the drawing.
After the blood was drawn, we would use the devise which was based, in principle, on Technicon’s hugely successful chemistry analyzers (“AutoAnalyzer). We were tasked with identifying blood and Rh type and the presence of unwanted antibodies. The antibody testing (Coombs’ test) line didn’t come with the equipment but was devised by Maples. He had also developed techniques to create our own reagents. Our work proved to be the most reliable and most economical in the entire Navy and we were visited by a group of Washington dignitaries, including a few Admirals, who wanted to see how we did it.
What brought me to these memories from more than four decades ago?
People whose knowledge bases are significantly deficient.
It is astounding to me that our country is being (mis)managed by people so obviously unfit for their responsibilities. I can’t tell you who should be labeled worst in the current administration—there are too many contenders—but my thoughts about Dudley were particularly awakened by the ineptitude, the gross incompetence, of RFK, Jr. (I find myself reluctant to use his given name since his father, Robert F. Kennedy, was such a hero for me).

Edward Jenner (1749-1823)
In 1798, the English physician, Edward Jenner, pioneered the concept of vaccination and invented the first successful preventative for smallpox, a terrible, often fatal, disease. After observing that young women working with cows infected with cowpox did not get the disease, he concluded that a similar, but far more lethal condition, human smallpox, might be used to induce resistance (“immunity”) to the disease. Last week, almost 250 years after Jenner, RFK continued to dismantle the National Institutes of Health (NIH) and its subsidiary organizations, including the Centers for Disease Control and Prevention(CDC). In case you didn’t notice, buried in the daily barrage of stupidity emanation from the White House, it was decided that most people under the age of 65 would not be eligible for the current COVID vaccine.
Almost at the same time, the Florida Surgeon General, has decided that mandates for vaccination of children will be discontinued in his state. He is supported by Florida’s deficient governor. It will be up to parents to decide if their children should be vaccinated. Madness! The Surgeon General asked, “Who am I to tell you what your child should put in [their] body?” I wanted to scream at the television: “You are a physician responsible for the health of those children, you idiot. That’s your job. That’s what doctors do!” But I immediately realized he would not understand. A graduate of the most prestigious medical school in the country, he seems to have missed the classes in public health and preventive medicine, the history of medicine, biostatistics (the data supporting the types of vaccination programs we have had until now is overwhelming) and integrity.
We should all be afraid, very afraid.
Understanding how Dudley got to his position is not that difficult. He did what he had to do and “kept his nose clean.” As far as I know, akin to the fictional Dudley Do-Right, he didn’t mean to harm anyone.
When the leader of an organization is uneducated, poorly informed, basically stupid, narcissistic and cruel, it should not be a surprise that the people he chooses to help him will share one or more of those traits, except that he will select people even less capable than he is. The widespread incompetence in this administration is terrifying. The cruelty makes it worse.
September 5, 2025 at 9:39 pm
You circle around trailing a lot of loose ends and then somehow tie them together and end up landing right on target! 🎯
September 6, 2025 at 11:46 am
Thank you. Hope you enjoyed it.
September 6, 2025 at 8:59 am
I have heard of unqualified people getting into positions of authority with a little luck and then charming others in positions of higher authority. The two people I have in mind spent most of their careers focusing entirely on promoting themselves and ignoring the careers of people underneath of them. In one case, the chair was an incompetent researcher. In the other case, the chair was an excellent teacher who did brilliant work for his PhD but then never undertook another project of much significance. Both were department chairs for decades. They caused great damage, but neither was involved in patient care. The people in their departments were mostly researchers who despised them. Neither of these people were pathologists. My guess is that when patient care is involved, the incompetence is usually impossible and too dangerous to ignore.
September 6, 2025 at 7:01 pm
very fascinating!! RFK(Dudley) especially.